

Vignesh Subramanian ’24
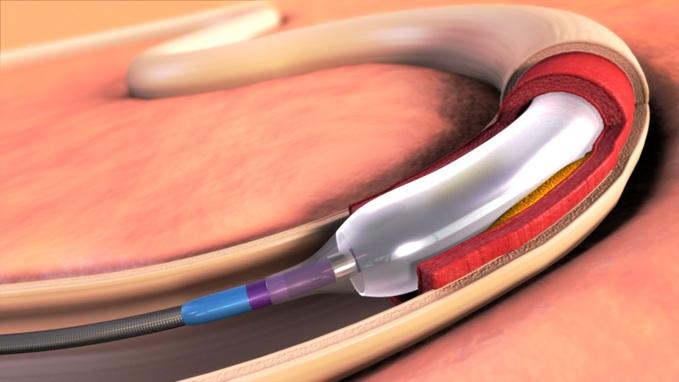
Intracranial atherosclerotic stenosis (ICAS) – the progressive narrowing of, and restriction of blood flow to, a major artery in the brain – is among the most common causes of ischemic stroke as well as recurrent stroke of any subtype. ICAS is responsible for the gradual obstruction of blood supply due to buildup of plaque within vessels, which is typically followed by excessive blood clotting due to local platelet activation. Clinical interventions aimed at preemptively circumventing blockages either prevent clotting – as combination antiplatelet therapy combined with management of risk factors aims to do – or else expand the passages available for blood flow. One means of accomplishing the latter is known as the percutaneous transluminal angioplasty and stenting (PTAS) procedure, which involves insertion of a balloon-tipped catheter that, when inflated, widens the vessel by pushing arterial walls outward, followed by implantation of a stent (a wired tube) that keeps the passageway open. To ascertain whether PTAS coupled with medical management was more effective at forestalling prognosis of stroke than solely medical management in a clinical trial for the first time, Stony Brook researcher Dr. David Fiorella and his team examined the rates of cerebrovascular accidents and mortality among high-risk patients.
Researchers deployed the PTAS procedure using the Wingspan Stent System – then the only FDA-approved device permitted to open narrowed arteries – in 224 subjects randomly selected from the pool of 451 patients who suffered recent transient ischemic attacks or stenosis-triggered stroke. Patients were administered clopidogrel, a blood thinner aimed at preventing stroke, as part of medication regimens and were operated on by neurointerventionists. Patients were then evaluated on the presence and severity of subsequent attacks in staggered intervals until 90 days after a primary endpoint, defined as stroke or death following enrollment or a revascularization procedure. Enrollment was eventually prematurely halted due to a heightened risk of periprocedural stroke or death being established in the PTAS clinical group. Researchers did have time to find that the probability of an early primary endpoint (within 30 days of patient enrollment) was significantly higher in the PTAS group than the uncoupled management group, with lower rates of stroke than expected appearing in the latter. The worsening of prognosis by PTAS application ultimately indicated that subsequent effects of the procedure’s stenting, which may include re-narrowing – the very issue it was designed to prevent – require further evaluation in the context of patients exhibiting high degrees of stenosis.
Works Cited:
[1] D. Fiorella, et al., Stenting versus Aggressive Medical Therapy for Intracranial Arterial Stenosis. The New England Journal of Medicine 365, 993-1003 (2011). DOI: 10.1056/NEJMoa1105335
[2] Image retrieved from: https://www.dicardiology.com/content/medtronic-drug-coated-balloon-tops-standard-balloon-angioplasty-landmark-study
